Clinical Presentation average age 15-30 years anovulation hirsutism infertility obesity virilization ...

Clinical Presentation
- average age 15-30 years
- anovulation
- hirsutism
- infertility
- obesity
- virilization
- most common pathologic finding: white, smooth, sclerotic ovary with a thick capsule, multiple follicular cysts in various stages of
atresia, hyperplastic theca and stroma


- but ovarian pathology varies and none is pathognomonic so diagnosis is biochemical
- fundamental defect = bad signals to hypothalamo pituitary axis:
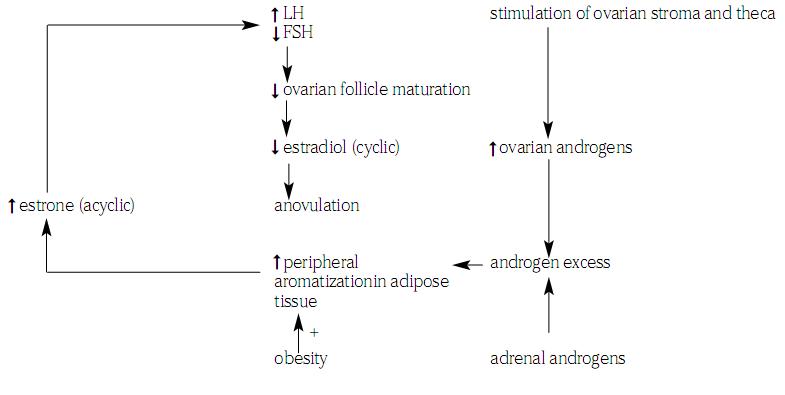
- increased incidence of endometrial cancer due to unopposed estrogen
Treatment
- interrupt the self-perpetuating cycle by:
- decreasing ovarian androgen secretion: BCP (wedge resections used in past)
- decreasing peripheral estrone formation: weight reduction
- enhancing FSH secretion: clomiphene, hMG (Pergonal),LHRH, purified FSH
- to prevent endometrial hyperplasia: progesterone (Provera), BCP
- for pregnancy
- medical induction of ovulation
- clomiphene citrate (Clomid)
- human menopausal gonadotropin (Pergonal)



